
Closing the Gap: Improving the Discharge Process for LEP Surgical Patients
Project Lead(s): Ryuta Fukuda, RN; Darcy McCarty, RN; Karen Trang, MD; Hannah Decker, MD; Alison Baskin, MD; Logan Pierce, MD; Elizabeth Wick, MD
Executive Sponsor: Pat Patton
ABSTRACT
Approximately 22% of adults in the United States speak a primary language other than English, and limited English proficiency (LEP) has been correlated with barriers to accessing to surgical care, increased risk of related adverse events, worse patient care experiences, and difficulty understanding of discharge instructions. Furthermore, LEP patients are more likely to have multiple other socioeconomic vulnerabilities, including employment, medical-legal assistance, health insurance, public benefits, lower health literacy, poorer housing quality and food insecurity. As we strive to ensure equitable surgical care is delivered to all, understanding the challenges, and developing mitigation plans for surgical patients with LEP is critical. At UCSF Health, about 11% of patients undergoing surgery have LEP and, while interpreter services are readily available and for the most part, utilized, evaluation of basic discharge metrics (LEP surgical patients discharge on average 1 hour later than non LEP counterparts) as well as informal discussions with nurses and providers suggests an opportunity for improvement.
This work is critical for multiple UCSF Health missions, including (1) quality and safety, (2) health equity (3) efficiency and financial strength (4) learning health system. Ultimately, if we can collectively improve in this area, beyond enhancing our performance on the True North Pillars, the UCSF general surgery and hopefully all surgical services will be national leaders in communication, surgery and the LEP patient.
TEAM
Department of Surgery: Elizabeth Wick, MD (Professor), Ian Soriano, MD (Associate Professor); Alison Baskin, MD, MPH (PGY 2 resident); Karen Trang MD (research resident and clinical informatics fellow); Sophia Hernandez, MD (PGY2 Resident) Hannah Decker, MD (Research Resident) Alexis Colley, MD, MPH (Research resident); TBD project manager
Department of Medicine: Logan Pierce, MD (Assistant Professor; medical informatics); Lev Malevanchik, MD (Assistant Professor)
Department of Anesthesia: Solmaz Manuel, MD
UCSF Health: Ryuta Fukuda, RN, Unit Manager 13L (and interim Unit Manager A5/6 MB); Darcy McCarty, RN, Assistant Unit Manager 13L, Toni Workman RN, DNP, Director Capacity Management, TBD RN 13L; Misti Meador, RN, Case Management; Nancy Huang PharmD Pharmacy; Shirley Darwish, RN PREPARE
Executive Sponsor: Pat Patton, Chief Nursing Executive, UCSF Health
PROBLEM
Improved operational efficiency and health equity are two priority areas for UCSF Health. Discharge timeliness data for LEP surgical patients lags that of English-speaking surgical patients across all languages. On discussion with the resident teams, frequently discharge instructions are either not provided translated into the patient's preferred language or translated with Google translation with questionable accuracy; there is no standard format or expectation. Instructions provided only in English mean that they can not be referenced later by the patient and family when questions arise. Providing patients written and verbal discharge instructions is in alignment with pre-existing UCSF practices to support all learning styles. Frontline nurses share that discharges can be delayed waiting for a family member who speaks English and cannot come during the day.
Importantly, more than 50% of the adverse events in surgery are diagnosed after discharge. Safe management requires patients and their families to recognize deviations from average recovery early and re-engage with their surgical team for management (“rescue”). After discharge, the burden of identifying adverse events is borne by the patient and family, and it is the healthcare system's responsibility to ensure that they are equipped to do this.
Over the past few years, to accommodate high capacity, particularly at the Parnassus Campus, emphasis has been placed on improving the efficiency of the discharge process. Early discharges on the surgical floors enable efficient daily operating room throughput. Even a one-hour delay in discharging a patient translates into extra recovery room minutes for another patient, which then cascades to additional operating room minutes for another patient. Operating room holds are costly and must be avoided both to improve value as well as ensure that highly specialized daytime teams can be leveraged for the most complex operations. Timely discharge of surgical patients also enables cohorting of patients on surgical floors, a practice that allows patients to benefit from specialty nursing as well as ease stress on provider teams. The efforts directed at timely (before noon) discharges have been productive over the past few years -- 13L is a high performer unit, but LEP patients have lagged. It is essential that we address this disparity.
This work is critical for multiple UCSF Health missions, including (1) quality and safety, (2) health equity (3) efficiency and financial strength (4) learning health system. Ultimately, if we can collectively improve in this area, beyond enhancing our performance on the True North Pillars, the UCSF general surgery and hopefully all surgical services will be national leaders in communication, surgery and the LEP patient.
Timely discharge of surgical patients is essential to maintain throughput through the operating rooms as well as enable cohorting of patients on surgical floors, a practice that allows patients to benefit from specialty nursing as well as ease stress on provider teams.
While 7.8% of the patients on the general surgery service have LEP, LEP patients are common on the surgical services at UCSF with some of the highest rates on CT, vascular and transplant (~12%).
TARGET
We aim to eliminate the gap in discharge by noon percentages between LEP and non-LEP surgical patients and ensure that 90% patients discharged with the top 5 most common general surgery and surgical oncology diagnoses receive discharge instructions in English and their preferred language.
GAPS
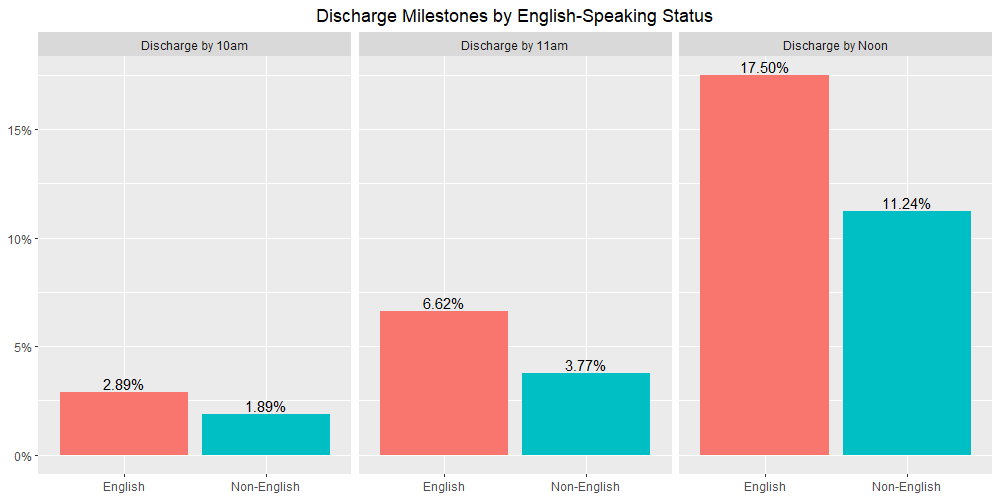
Data demonstrates discharge inefficiencies are consistently noted in LEP surgical patients at UCSF, with under 12% of LEP patients being discharged before noon (compared to 17.5% of English-speaking patients). The data is corroborated by frontline providers and nurses reporting frequent challenges with accurate discharge instructions, coordinating with family members and last-minute changes. This is prevalent on 13L (top) as well as all units (bottom).
INTERVENTION
With this caring wisely proposal, we aim to improve the efficiency and quality of the discharge process for surgical patients with LEP.
To achieve this goal, we will:
Aim 1: Understand the Current State and Identify Opportunities for Improvement
We will use a combination of approaches to understand the current state, including interviews with key stakeholders (patients and families, nurses, social workers, case managers, and providers) and observation of LEP and non-LEP surgical patient discharges. While the focus will be on the 24 hours around the time of discharge, there may be an opportunity to better anticipate needs preoperatively (for scheduled operations) or earlier in the hospital stay (for urgent/emergent operations); therefore, before identifying the 2-3 potential small tests of change, we will convene stakeholders along the continuum of surgical care for 1-2 sessions to further review findings and ensure all opportunities for improvement are considered.
Aim 2: Improve Language Concordant Standardized Discharge Instructions
We will work collectively (incorporating the perspective of provider and nursing teams as well as patients and families) to develop a strategy to standardize discharge instructions for common general surgery and surgical oncology procedures. One approach may be to have a core set of instructions that applies to multiple procedures with specific additional modules for conditions like wound care, drains, ostomies etc. Whatever the agreed-upon approach, the instructions will be agnostic of the surgical attending, written at the 6th grade literacy level, and translated into Spanish, Chinese and Russian (the most common languages seen on the 13L). To ensure they are easily accessible to all providers, we work with the APeX clinical documentation team to embed them in the discharge navigator.
Aim 3: Implement 2-3 small tests of change aimed at mitigating a barrier to discharge identified in aim 1.
While preparing this proposal, solutions have been proposed to improve the discharge process for LEP surgical patients. However, given the diverse set of stakeholders and importance of considering all perspectives, we will identify 2-3 small tests of change based on the work completed in aim 1. We anticipate conducting each experiment for 2 months and expect each change will be an iteration of the previous. However, we are receptive to the idea that we may need to go back to the drawing board and pivot entirely. Ideas floated include arranging “appointment times” for discharge teaching with designated family member, staged discharge teaching, early completion of discharge paperwork for LEP patients with close communication between 13L and provider teams. But, importantly until we convene all stakeholders, we don’t want to “solution.”
We will develop a simple dashboard to proactively identify LEP surgical patients on 13L and monitor agreed-upon performance metrics. This will be essential for rigorously evaluating each test.
The work will be integrated into the 13L UBLT leader rounds as well as daily huddles and shared in the weekly general surgery provider meetings. Anticipated barriers include time, resistance to standardizing workflows, dissemination of information and clunky workflow but we believe that, with time, the transdisciplinary collaboration between the provider team and frontline nursing as well as leadership support, we will be able to improve. Beyond the impact of improving the discharge process for LEP surgical patients, enabling surgical resident and frontline nurses to closely collaborate via dedicated non-clinical time has the potential to promote broader enhancements in safety culture and teamwork on the unit that will positively impact all patients.
TIMELINE:
Aim 1: July-August-September
Aim 2: August-September-October (may need to adjust later in the year, pending aim 3)
Aim 3: October-November-December (Test 1); January-February-March (Test 2); April-May-June (Test 3)
Sustainability and Spread Planning: May-June
PROPOSED EHR MODIFICATIONS
- What are the clinical problems you are hoping to solve with APeX?
- Discharges instructions are frequently in English or translated by Google, limiting the accuracy and utility of discharge instructions for patients and families with LEP. Discharge instructions are an important reference for both RN teaching as well as for patients and families to references in the event of complication at home.
- What APeX tools (patient lists, reports) or workflows (orders, documentation, alerts) are you using now to achieve this goal? How would you want these modified?
- Using many personalized dot phrases for discharge with translation by Google with questionable accuracy.
- What new APeX tools/workflows do you think you need to achieve the goals of your project?
- We are hoping to develop 3-5 discharge instructions for common general surgery and surgical oncology procedures that are in English, Spanish, Chinese and Russian.
- To increase ease of use, we would like to embed them in the General Surgery SVC discharge navigator
COST – We estimate the cost for the work to be ~$50,000. Many of the personnel involved in the project will donate their services or are funded by other projects that are very much aligned with this work (H. Decker, R. Fukuda, D. McCarty, E. Wick).
SUSTAINABILITY - Collectively, this work will take critical first steps to improve the discharge process for LEP patients undergoing surgery. Likely, we may also identify opportunities that could have a positive impact on non-LEP surgical patients. Spreading new practices to all patients could make transitioning from “special project” to routine care easier. Given that discharge by noon is a regularly followed metric, with strong performance on 13L, we will explore the potential of adding discharge by noon by LEP vs non-LEP to the 13L metrics to ensure the work will have additional visibility. We will leverage the 13L UBLT and the newly founded Perioperative Quality and Safety Council for both spread beyond the Department of Surgery and accountability. We have also include experienced champions from hospital medicine and anesthesia (Lev Malevanchik and Solmaz Manuel) to ensure that our efforts align with other departments, reinventing the wheel is avoided and we can breakdown silos.
Furthermore, we have assembled an outstanding trans-disciplinary team, with engaged executive sponsorship, that has the potential to ensure alignment with UCSF Health throughput efforts (and avoid re-inventing the wheel), facilitate the spread and if needed, address barriers encountered.
The proposed work will occur in conjunction with related work in surgery including further supporting the sustainability of the work:
(1) UCSF surgical resident GME incentive project to create and pilot language concordant discharge instructions from 3-5 common general surgery procedures at Parnassus.
BUDGET -
- 1. Gift cards to acknowledge patient and provider participation in interviews and focus groups (25 @ $40/card = $1,000)
- 2. Translation Services ($5,000)
- 3. Stipend for resident leaders ($6,000)
- 4. Party to celebrate achieving interim and final goals ($1,000)
- 5. Non-clinical time for stakeholders to attend 2 – 2 hour sessions to ($10,000)
- 6. TBD RN from 13L 4 hours per week to interview patients and families, collaborate on interventions, educate and train unit ($15,000)
- 7. Logan Pierce, MD, Assistant Professor of Medicine, Clinical Informatics, Department of Surgery, data and analytics (5% effort, $12,000)
{kind=link}
{kind=link}
Comments
Very important work and
Very important work and excellent proposal that will benefit patients!
This is incredibly important
This is incredibly important work that will have tremendous benefits for patients and providers alike. It also demonstrates the impact that residents can have in driving research and clinical change, and also shows that collaboration between nursing and surgery can be be extraordinarily fruitful.
This proposal touches a way
This proposal touches a way to improve efficiency and quality of perioperative care among minority patients having limited English Proficiency. Very well written and impactful to addressing real world disparities in health care.
We can truly provide better
We can truly provide better care for this population of patients thru this collaborative project between faculty, nursing, and residents. The data is clear that this population of patients require more resources to provide comparable care to primary english speaking patients.